What unit dose packaging means in real hospital operations
A unit dose system is not just “small packets.” It is a pharmacy-coordinated distribution model where medications are packaged as single units, dispensed as ready-to-administer as possible, and (for most meds) only up to a 24-hour supply is kept available in the patient-care area. This is why it is often discussed as a hospital-wide control system—not merely a packaging choice.
From an industry glossary perspective, a “unit dose packaging system” is a medication delivery method using pre-measured drugs in secure packages, commonly used for oral meds in hospitals.
Hospitals frequently implement unit dose through “unitarization”: repackaging and labeling medications so they can be issued to wards with hospital-ready identification and traceability. OpusPac describes unitarization as preparing drugs in ready-to-administer form, typically under hospital pharmacy responsibility, combining packaging and label printing.


Benefits by stakeholder group
At the macro level, the case for unit dose is driven by the scale of medication harm: World Health Organization estimates medication errors cost about $42B annually worldwide and set a goal to reduce severe avoidable medication-related harm by 50% globally. For hospital leaders, unit dose is one of the practical “system interventions” that strengthens weak medication-use processes (dispensing, administration, monitoring) where errors concentrate.
For patients, the most direct benefit is fewer dispensing/administration errors through standardization and scan-enabled verification. In a before/after study in an inpatient ward at Helsinki University Hospital, introducing unit doses reduced medication errors from 3.2% to 1.7% and procedural errors from 37.4% to 13.9%, while barcode-scanning problems dropped markedly.
For nurses, unit dose reduces “medication-related activities” and supports bedside confidence when paired with barcode workflows. Canadian Society of Hospital Pharmacists explicitly links unit-dose/I.V. admixture models to decreased medication-related work for nursing, more efficient use of staff, and improved job satisfaction. The same Helsinki ward study found barcode scanning improved after unit-dose introduction—important because scanning adherence is a key layer of bedside safety.

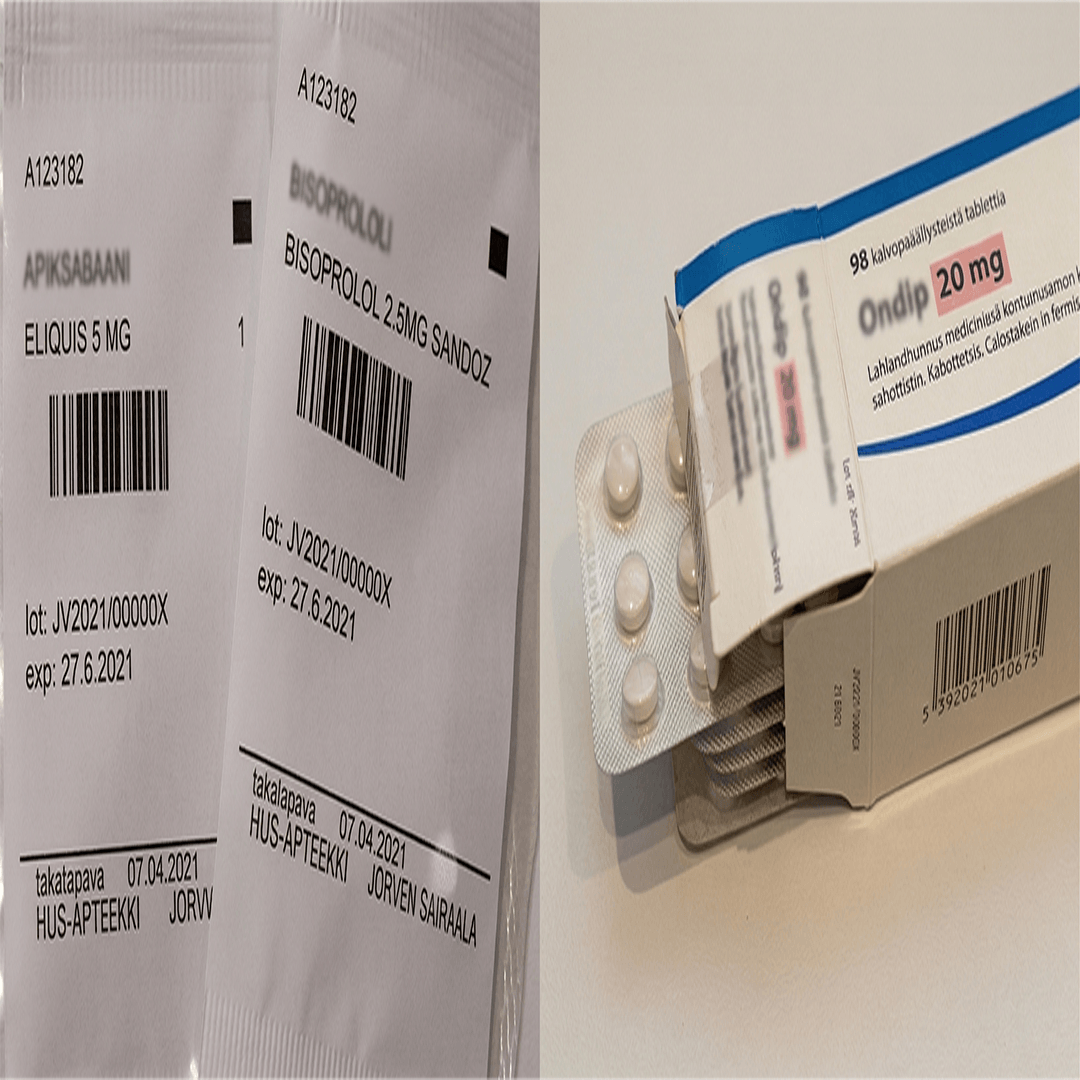
For pharmacists and pharmacy management, unit dose centralizes control and strengthens monitoring. A core advantage cited in the unit-dose distribution statement is improved drug-use monitoring and reduced medication errors versus alternative distribution methods. In unit-dose packaging guidance for hospitals, critical operational goals include precise content identification, environmental protection (light/moisture/handling), and labels that clearly carry key data such as drug name, dose, and expiration date—controls that support safe dispensing and audit readiness.
For inpatient wards and clinical staff, unit-dose distribution reduces ward stock complexity: floor stocks are minimized and limited mainly to emergency and routinely used “safe” items under the hospital distribution model described in technical guidance. This is a practical safety gain because it reduces selection errors and removes informal “workarounds” created when wards manage bulk packs.
For management and the finance division, unit dose has measurable cost-control mechanisms: more accurate patient billing, minimized drug credits, smaller ward inventories, reduced wastage/pilferage, and improved activity-based costing through patient-specific accounting. On the payment logic, industry descriptions also note unit dose can accommodate paying for only the amount needed (reducing waste driven by bulk dispensing).
Accuracy, safety, and compliance controls that leaders should require

Accuracy is not a slogan—it is engineered through labeling standards, verification steps, and scan-enabled workflows.
At the system level, unit doses enable electronic documentation by barcode scanning and reduce manual, error-prone steps in medication handling. When implemented with barcode medication administration, evidence summaries from Agency for Healthcare Research and Quality describe BCMA as a method to reduce administration-phase errors and support the “five rights” of medication administration. Closed-loop medication management frameworks similarly emphasize replacing manual steps with technology across prescribing-to-administration, while also noting that new technology must be managed carefully because it can introduce new operational challenges and costs.
At the packaging and labeling level, hospital leaders can align unit-dose policy with regulatory safety logic: European Medicines Agency highlights that medication-error risk is influenced by pharmaceutical design, including packaging and labeling, and recommends careful design to minimize mix-ups between products. Unit-dose packaging guidance for hospitals also emphasizes that each package should identify contents precisely, protect contents from environmental factors, and display critical data like expiration date and control identifiers—practical controls that strengthen compliance during recalls, audits, and incident investigations.
At the process level, “unitarization” needs disciplined controls: dedicated space, hygiene, one product/batch at a time to prevent mix-ups, and barcode-based traceability. Finally, sustainability is a leadership consideration: the Helsinki study reports staff concerns about plastic waste, which should be addressed through procurement choices and waste-reduction planning.
Deployment models and example equipment features
Most hospitals choose one of three unit-dose deployment models, often in phases.
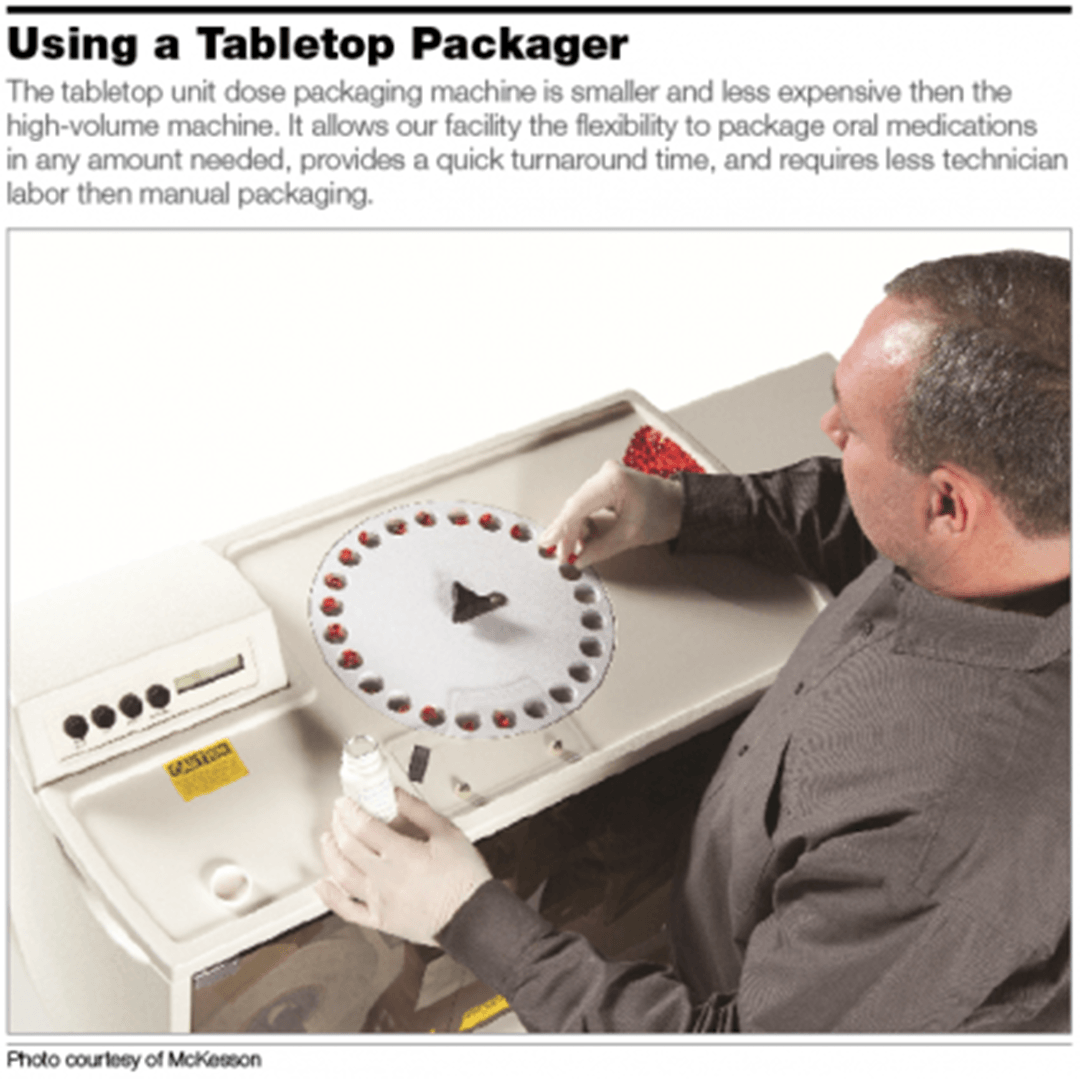
Model one is manual or semi-manual unitarization: pharmacy-controlled repackaging/labeling, often performed soon after medicines are received to standardize identification before ward distribution. Model two is centralized automated strip/label packaging in the hospital pharmacy, emphasizing consistent print quality (dose, expiry, barcode) and inventory traceability. Model three is integrated “closed loop” automation: unit dose + automated dispensing cabinets + eMAR/BCMA, aligning dispensing and administration verification.
Equipment capabilities matter because they operationalize accuracy. Euclid Medical Products describes the Industrial Cadet as packaging up to 50 units per minute and highlights barcode capability, “complete sensors,” and 300 dpi thermal printing; it also lists options like fingerprint reader, pill camera, and barcode scanners, plus software features such as customizable reports and password protection—features that support audit trails and controlled access. The same vendor also positions a fully automatic liquid unit-dose platform (Speedy Wet Cadet) for unit-dose liquids, which is relevant if your inpatient formulary includes oral syrups or other liquid dosing.
For high-volume tablet dispensing and pouch packaging, JVM materials describe systems that combine speed and inspection: MENITH is described as producing about 120 pouches/minute and (optionally) using an internal inspection system that stores inspection results in image/data formats; it also highlights automatic canister recognition using RFID tags (supporting tracking and expiry-first use) and customizable pouch print layouts (including barcode and expiry data). JVM’s ATDPS materials similarly describe selectable pouch sizes, RFID/ACRS-based canister recognition for inventory control, and separate packaging when incorrect tablets are detected—features that directly support accuracy and exception handling.

FAQ and executive call to action
Does unit dose packaging measurably reduce errors?
Evidence includes ward-level reductions in medication/procedural errors after unit-dose introduction, and systematic-review findings describing substantial error reductions when automated unit-dose systems are integrated with barcode workflows (while also noting the evidence base is limited and implementation-dependent).
What are the advantages of governance for executives?
Unit-dose distribution narrows uncontrolled ward inventory supports patient-specific medication profiles and improves billing and drug-use monitoring—core levers for clinical governance and financial stewardship.
What compliance controls should be non-negotiable in an RFP?
Per-dose identification (drug, strength, expiry), barcode-readable labeling, packaging that protects contents, controlled access/audit trails in software, and a documented process that prevents mix-ups (one product/batch at a time, inspection, traceability).
How should large hospitals phase implementation to protect operations?
Closed-loop reviews emphasize staged adoption and change management because technology changes workflows and can create new risks if not governed.
CTA (for large clients):
If your organization is planning a step-change in medication safety, workforce efficiency, and financial control, unit-dose distribution plus barcode-enabled workflows is a proven operating model endorsed by hospital pharmacy bodies and aligned with global medication-safety priorities. We invite large hospitals and multi-site health systems to join hands with us to design and implement a unit-dose packaging program tailored to your formulary, ward workflows, compliance needs, and growth plans—because in practice, the best outcomes come from customization, integration, and disciplined operational governance.